Confirm Comorbidities
Review the information below and confirm if your patient has one or more of the conditions listed. If you do not have a confirmed diagnosis, consider the recommended investigations, where appropriate. Select all conditions that apply then continue to risk staging.
Outputs are tailored based on the combination of conditions selected.
Advanced Chronic Kidney Disease:
- Patients who are ≥ 65 years and/or are frail or have comorbid illnesses such as HF, are at high risk for poor outcomes and are appropriate for this pathway
- Advanced CKD eGFR category 4 and 5: 2 eGFRs ≤ 29 ml /min/1.73m2 ≥ 90 days apart AND have a comorbid illness such as HF
- This pathway uses a Conservative Kidney Management (CKM) approach. CKM is a treatment option for managing kidney disease with a focus on a quality of life, symptom management, and living well without dialysis
Advanced stage cirrhosis: Child-Pugh B or C
- In patients with risk factors for chronic liver disease, AST, ALT, and platelet count can help rule out cirrhosis
- A FIB 4 (calculated using age, AST, ALT and platelet count) cut-off score of < 1.3 is a good predictor of the ABSENCE of cirrhosis in all clinical contexts
- As per the AHS Fatty liver pathway, if your patient has a FIB-4 of ≥ 1.3, refer to a liver specialist
- Elastography is a good tool to assess liver fibrosis. Normal results of elastography can help rule out cirrhosis and values > 15 kPa (by transient elastography) strongly suggest cirrhosis
- A low platelet count (<150 G /L) is an important clue that a patient may have cirrhosis
- Patients with suspicion of cirrhosis based on the above-mentioned tests should be referred to a liver clinic
- In unclear cases, invasive tests (liver biopsy, hepatic venous pressure gradient measurement, endoscopy) will be required to come to a final diagnosis

Cancer:
- Stage 3 or 4, metastatic solid organ cancer
- Cancer is non-curative
- If patient is on active treatment, including palliative intent therapy, or is being actively followed by a Cancer Care Alberta oncologist, contact the patient's Cancer Care Alberta team before using this tool or starting medical management
- For urgent issues, follow the instructions on the patient's systemic therapy or checkpoint inhibitor therapy emergency contact card

COPD diagnosis confirmed with post-bronchodilator spirometry with FEV1 to FVC ratio < 0.7. Moderate to severe COPD: defined as <50% FEV, mMRC> 2; +/- hospitalization/ED visits
- Chest x-ray at initial diagnostic evaluation
- 02 saturation (if < 90% at rest, consider ABGs for home 02)
- Document BMI (low BMI may dictate need for nutritional support)
- Assess for comorbid illness (depression, cardiac disease, diabetes etc.)
HF investigations: ECHO, NT-proBNP, Creatinine, eGFR, electrolytes
- HF may occur with any degree of LVEF. However, evidence for therapies and treatment targets are based on whether LVEF is 40% or less HF with HFrEF or > 40% HF with HFpEF
- If recent hospitalization for diagnosis or decompensation of HF, ensure NT-pro-BNP and ECHO with documented LVEF have been done
- Creatinine/eGFR, and electrolytes - regular monitoring to establish baseline and guide pharmacotherapy
Final Weeks and Days of Life
General Considerations
Patients in the final weeks to days of life require careful assessment and management. They may have ongoing physical, emotional, spiritual and social distress, and may not be able to clearly communicate their needs. Provide the patient and caregiver with resources about what to expect in the final weeks and days of life.
- Although these can be re-addressed at any time at the provider’s discretion or request of the patient/alternate decision maker(s), any significant change in patient’s condition or location of care should trigger a re-evaluation of the patient’s goals, wishes and priorities and goals of care
- Review all previous advance care planning, goals of care, or serious illness conversation documentation
- Personal directive – including naming of Agent
- Goals of Care Designation form
- ACP/GCD Tracking Records
- Clear and compassionate communication about prognosis to allow patient and family to express their hopes, fears and goals for end-of-life care
- Gentle inquiry of the patient and family about what a “good death” represents for them
- Gentle inquiry of the patient and family about cultural or religious beliefs and rituals pertaining to the end of life
- As the patient’s condition declines and physical symptoms increase, goals may shift. Life prolonging interventions may no longer be in line with the patient’s goals or they may no longer be medically appropriate. The patient may choose to focus more on comfort and symptom management. Ideally, these conversations should take place with the patient. If the patient has lost capacity, however, decisions should be made with the appropriate alternate decision maker
- Use of a tool such as the Serious Illness Conversation Guide can greatly enhance the quality of these conversations
- Ensure CPR discussions have taken place and agreement is made regarding No CPR. This must be clearly documented
- Discussion and deactivation of cardiac implantable defibrillators
- Place of death
- Organ donation
Certain non-pharmacological interventions will become unrealistic (e.g. exercise).
- Energy conservation will become more important
- Ensure that appropriate supports (e.g. home care including nursing care to monitor symptoms and coordinate care) are in place to assist with activities of daily living, and psychosocial-spiritual needs
- Consider ongoing discussions with patient and alternate decision maker(s) to address goals of care as condition and prognosis change
General Principles
- Consider medication availability and routes of administration options at the location of care
- In accordance with goals of care decided with the patient or alternate decision maker(s), when appropriate, review all medications and prioritize essential medications for symptom management and quality of life
- Deprescribing needs to be individualized to the clinical situation. Specialists and pharmacists can help to determine the medications that can be stopped first
- Near the end of life, oral medications may no longer be an option
- Intravenous routes are also not an option in home, hospices or nursing homes
- The subcutaneous route is often the best choice in the last week to days of life
- Ensure an adequate supply of injectable medications for those at home. 24/7 nursing support at home (even through home care) is not always possible. It is important to remember that family members might be the individuals drawing up syringes and administering medications. Simplify the number and frequency of medications, if possible. Consult palliative specialists or pharmacists for advice, if needed
- Carefully weigh the benefits and risks/side-effects of the medications used for symptom management and comfort. When appropriate, some “side-effects” of medications may actually provide benefit; choose medications carefully
- Careful history taking and physical examination should continue to rule out medication induced side effects
- Careful and gentile history taking to ensure medications are stored safely in the home (especially opioids and narcotics)
- For morphine and hydromorphone, conversion from oral to subcutaneous administration is to divide the oral dose by 2. (i.e. 1mg SC is equivalent to 2mg PO)
- Example 1:
- A patient has been on hydromorphone sustained release 12mg PO q12h and hydromorphone short acting 2mg PO q1h prn
- She has now lost her ability to swallow and needs the hydromorphone administered subcutaneously
- Over the past 3 days, she has consistently used 3 PRN doses per 24 hours
- Step 1: Calculate the total daily hydromorphone oral dose administered
- (12mg x 2) + (2mg x 3) = 24 + 6 = 30mg in 24 hours
- Step 2: Calculate the total daily hydromorphone subcutaneous that will need to be administered
- Subcut is twice as strong as oral, so we divide the oral dose by 2
- 30mg oral / 2 = 15mg subcut
- Step 3: Divide the total daily hydromorphone subcutaneous dose by 6 for q4h dosing of the short acting parenteral preparation
- 15mg / 6 = 2.5mg subcut q4h
- Step 4: Also order the breakthrough dose subcutaneously
- Breakthrough doses are usually 10% of the total daily
- Total daily is 15mg subcut, so 10% would be 1.5mg
- Breakthrough dose would be: 1.5mg subcut q1h prn
- Step 1: Calculate the total daily hydromorphone oral dose administered
- Example 2:
- A patient has been on morphine short acting for dyspnea, using 5mg q6h regularly and 2.5mg q1h prn
- He is likely to lose his ability to swallow and we are preparing subcutaneous orders
- Over the past 3 days, he has only needed 1 PRN dose 2 days ago. So, we will not include any PRN doses in the conversion
- Step 1: Calculate the total daily morphine oral dose administered
- 5mg x 4 = 20mg in 24 hours
- Step 2: calculate the total daily morphine subcutaneous that will be administered
- Subcut is twice as strong as oral, so we divide the oral dose by 2
- 20mg oral / 2 = 10mg subcut
- Step 3: Divide the total daily dose into q6h doses (q4h dosing for some patients is appropriate; but in this case, since the patient was doing well on PO q6h, we will keep the subcut to q6h as well)
- 10mg / 4 = 2.5mg subcut q6h
- Step 4: Also order the breakthrough dose subcutaneously
- 10% of total daily of 10mg = 1mg
- Breakthrough dose would be: 1mg subcut q1h prn
- Step 1: Calculate the total daily morphine oral dose administered
- Example 1:
- For metoclopramide, haloperidol, dexamethasone, or lorazepam, the subcutaneous dosing is the same as oral, with the same dosing interval as well. (i.e. if the patient has needed haloperidol 1mg PO q8h, when they lose their swallow, can order haloperidol 1mg SC q8h)
Investigate for the cause of symptoms only if it's necessary to promote comfort, or add to targeted symptom management
- Most medications targeting neuropathic pain are not available as injectables when subcutaneous route needed (e.g. gabapentin). A switch to opioid medication or titration of existing opioid doses will likely be necessary
- Given the focus on comfort, CNS side effects are often not as critical for patients. Good discussions are important. Faster titration of medications may result in more CNS depressant effects, which may be aligned with patient goals
- Patients usually require subcutaneous medications or alternative routes of administration of analgesics at the end of life when they lose the ability to swallow
- A history of substance use may affect the dosing of medications required at the end-of-life and may make the patient and family more reluctant to use opioids. Specialist consultation may be required
Consider non-pharmacological management in all patients where breathlessness has a significant impact on patient’s quality of life or function
- At End of life, as the patient’s condition deteriorates, opioid titration will likely need to be escalated for dyspnea
- Consider Palliative Care consultation as required
- As a patient’s condition deteriorates, sodium and fluid restrictions should be discontinued. Similarly, consider discontinuing hypodermoclysis when a patient has days-to-hours to live
Upper airway congestion is unlikely to cause distress to patients, who are usually unresponsive at this point. However, it may be a source of distress to family members at the bedside
- Discuss with family members about the cause of the upper respiratory secretions
- It is not indicative of any choking or drowning risk
- Non-pharmacological approaches are important
- Repositioning of the patient, reassessment of fluid volumes, and possibly gentle suctioning can be considered
- Antimuscarinic agents can help to reduce this distressing symptom, though emerging evidence suggests the timing of their initiation may impact effectiveness
- When needed, it is best to begin them early – prophylactically
- Choice of antimuscarinic agent often depends on local availability and patterns of practice, but those that cross the blood-brain barrier will be more likely to increase sedation which may be pertinent in the clinical context
- These medications are often included in the end-of-life care pathways available at many institutions (and in the ‘C2’ order set in Connect Care)
- Patients continue to produce stool until the last hours of life. If no bowel movement, stimulant suppositories may be required every 3 days to prevent abdominal discomfort
- As a patient’s condition deteriorates, certain pharmacological or non-pharmacological interventions will become less realistic; if the patient has hours to short days to live, consider discontinuing bowel care if there are no obvious symptoms arising from constipation
- As a patient’s condition deteriorates, certain non-pharmacological interventions will become less realistic (e.g. exercise). Energy conservation and restoration will become of utmost importance
- Ensure that appropriate supports are in place to assist with activities of daily living and that nursing care is available as needed
- Drowsiness may increase as the end of life approaches due to disease progression (and/or medications). Some patients and families may even prefer increased sleepiness if the patient remains comfortable

Benzodiazepines
- Benzodiazepines are not a first line treatment for Restless Legs Syndrome but there is some limited evidence for their use. Benzodiazepines can carry significant risks including an increased risk of falls/fractures and decreased cognition. If the patient is experiencing refractory Restless Legs Syndrome causing significant sleep disturbance, or if benzodiazepines may potentially treat concurrent symptoms (e.g. anxiety), they could be considered. They may also be the only option for a patient who is no longer able to swallow
- Prescribers could consider initiating midazolam 1 mg subcutaneously q4h PRN
- Some drugs commonly prescribed at end of life, such as haloperidol and opioids, may potentially contribute to Restless Legs Syndrome
- Evaluate potential etiologies and discuss with patient/alternate decision maker. The likelihood of being able to determine a cause of the delirium becomes much less as a patient approaches the end of life
- For severe agitated delirium at the end of life and when goals are comfort focused, palliative sedation can be considered (e.g. continuous midazolam infusion). A Palliative Care specialist consultation is highly recommended for this
- At End of life, as the patient’s condition deteriorates, anorexia will worsen and it will not be amenable to therapy (including enteral/parenteral nutrition)
- Discussions around eating for pleasure may help patients to be able to balance adverse effects versus benefits at this stage
- If anorexia or conversations around the utility of nutritional therapy at end of life are of particular distress for the patient, family or team, a consultation from Palliative Care should be obtained
- As the patient’s condition deteriorates, muscle cramping may worsen and not be amenable to the recommended therapies
- If muscle cramps are causing significant pain, pain medication may be required
- Discuss with the patient and family that pharmacological therapy may increase drowsiness
- Consider Palliative Care consultation for refractory symptoms
Continue to consider Palliative Consult Team involvement if there are ongoing issues around symptoms or location of care
-
- Pain or other symptom management remains suboptimal despite approaches described in guidelines
- An opinion about safety and limits of therapy is needed
- Assistance with management of Total Pain (or other symptom) Syndrome is needed
- Intensive (Tertiary) Palliative Care Unit admission or Hospice placement is required
- Practitioner uncertain about any of the above steps
- Multi-system complexity, including pain
- Patient or family psychosocial distress compounding the pain or symptom experience
- Complex advance care planning or goals of care delineation
- In urgent situations in the patient’s home, front line paramedics and community clinicians work together to ensure that the management of the emergency (including symptom crisis) matches the patient’s wishes and care plan. This may include providing support to patients in their homes (including nursing homes) rather than transporting to a hospital
- The most responsible healthcare provider (MRHP) has to ensure that the patient is registered with Home Care (HC), and has to work closely with HC to ensure that the patient and family are fully prepared, and receive adequate support to enable a death at home. The MRHP is usually the patient’s family physician or a nurse practitioner acting as MRHP, and need to be involved for a successful death in the home
- If goal is to achieve a supported death at home, home care nursing will ask MRHP to collaborate on the completion of a Expected Death in the Home form
- (Zone dependent) may need referral to palliative care consult team (or palliative home care) for hospice waitlisting
- Nursing considerations
- Mouth care
- Frequent turns and repositioning
- Management of medications and non-oral routes of administration
- Education for family and caregivers
- Reduction or discontinuation of vital signs monitoring
- Preparation of death at home
- Expected Death in the Home Form
- Back-up plan – hospice or alternate location of death if a supported death at home becomes non-feasible
- Pronouncement of a patient’s expected death at home is not required; the patient’s attending physician (e.g. family physician) certifies the death by completing the Government of Alberta Vital Statistics Attending Physician’s Medical Certificate of Death Form within 48 hours of the death unless the death is notifiable as per the Fatality Inquiries Act
- The physician can refer to public health guidelines for reportable deaths depending upon location/province
One:carepath Handout Preparing for the End of Life
AHS Palliative and End of Life Care
AHS EMS Palliative & End of Life Care Assess, Treat and Refer
AHS Patients Death in the Home Care Setting
AHS Bereavement Care Resources
Pilgrim Hospice Society Grief Support Programs
My Health AB - Grief Counselling
Inform Alberta Local Bereavement Support Groups
Canadian Mental Health Association (CMHA) Grieving
Frailty
Frailty assessment can provide additional information to inform shared decision-making and lead to individualized management suggestions, such as a shift to conservative care or liberalization of dietary restrictions. Given the high prevalence of frailty in younger people with ESKD, the role of early identification and the impact of frailty on transplant eligibility provides a strong rationale for advocating frailty assessment in younger, fitter patients.
Once you have risk stratified consider Frailty Screening using the Clinical Frail Scale (CFS)
Top Tips to help you use the Clinical Frailty Scale
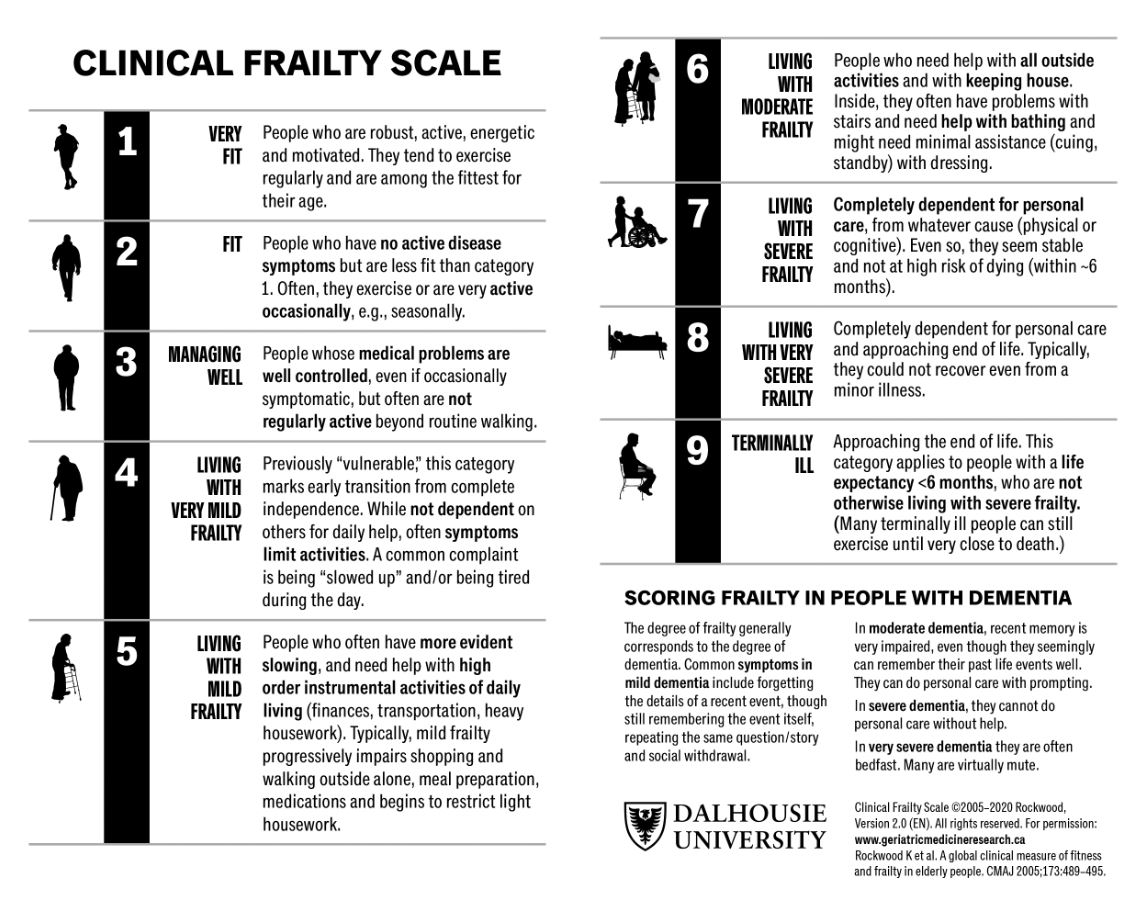
- Patients with severe frailty are approaching end-of-life
- Focus on conservative management and end-of-life planning
- Review/update advance care planning discussions and goals of care designations
- Consider referral to comprehensive geriatric assessment
- Review “yes/no” screening questions to determine frailty domains